
{kind=link}

[ad_1]

[This post has been co-authored by Swaraj and Sabeeh. Long post ahead]
Cancer incidences continue to increase in India, with over 1.46 million estimated new cases diagnosed annually as of 2022 and predicted to rise to 1.57 million cases by 2025 (More on these numbers later!). The continuous interaction of public health priorities with IP laws have been mainstream discussion for a long time now. To what extent exactly do IP laws create, shape, or impact the political economy of the cancer treatment landscape in India? Pursuing these questions, we started by trying to understand the existing landscape and focussed on preliminary data collection of relevant cancer and their associated drugs. Some baseline data such as cancer incidence, approved drugs, and associated patents, etc. is needed to begin with. To put it mildly, this turned out much more difficult than we thought it would be. We expect to come across more conceptually complex issues through the course of this journey, however for now, the purpose of this post is to simply narrate the difficulty in locating what data is available, and how the absence of primary data affects the larger cancer treatment landscape. And on that same note, as will be made abundantly clear, we are not certain about any of this data being the final word in what they cover! So we also request that anyone who has more information, or knows where we may get more information, please let us know in the comments below!
Where Do You Get the Data From? – Cancer Incidence and Burden
For current purposes, we were looking at the 5 types of cancer with the highest incidence rates in India. These include lung, breast, colorectal, oral, and cervical cancer. How much exactly is the disease burden though? One may assume this would be easy to get, and that there would be a reasonably well maintained public database or registry that records cancer incidences in the country. But that isn’t exactly the case.
The National Cancer Registry Programme (NCRP) at the ICMR-National Centre for Disease Informatics and Research (NCDIR) is the official database that records cancer incidences in India. It uses its network of 38 geographically spread Population Based Cancer Registries (PBCR) and Hospital Based Cancer Registries (HBCR). (PBCRs collect cancer incidences in defined geographical locations, whereas HBCRs record information on cancer incidences in a particular hospital irrespective of where the patient population belongs to. The data collected under HBCRs also contribute to respective PBCRs). The last NCRP Report came out in 2020, and it covers the period between 2012-16.
This 2020 report stated that PBCRs cover close to 10% of the population in India and further projections are made on the basis of this data. As a case study, we started looking specifically for lung cancer data. The projections for 2020 and 2025 were 98278 and 111328 cases (incidences) respectively. Now, the primary drawback to this projection is that the methodology assumes a constant incidence rate for the future. The 2020 report states that ‘The influencing factors such as risk factors/behaviour, case finding procedure, screening programme, improved technique for detecting cancer patients are likely to influence the projection of cancer cases.’ The Cancer Samiksha portal also seems to be using the same data source, as the results within the portal leading to a PBCR dashboard match with the 2020 NCRP report. An interactive map on the Cancer Samiksha portal attempts to provide numbers from individual PBCRs but again the data is either not published or from the 2020 NCRP. There is no other public official Indian database that we could find for these numbers.
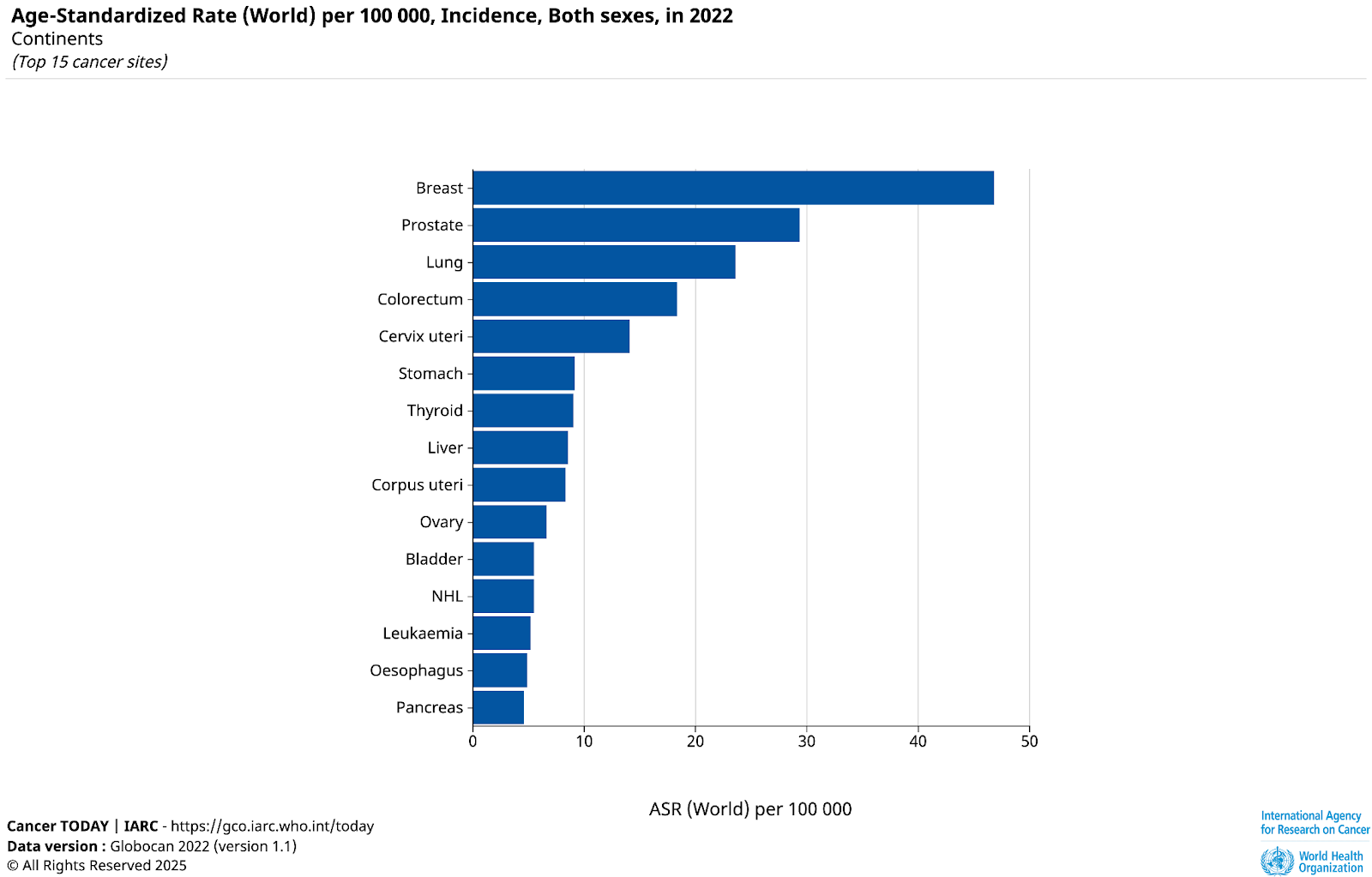
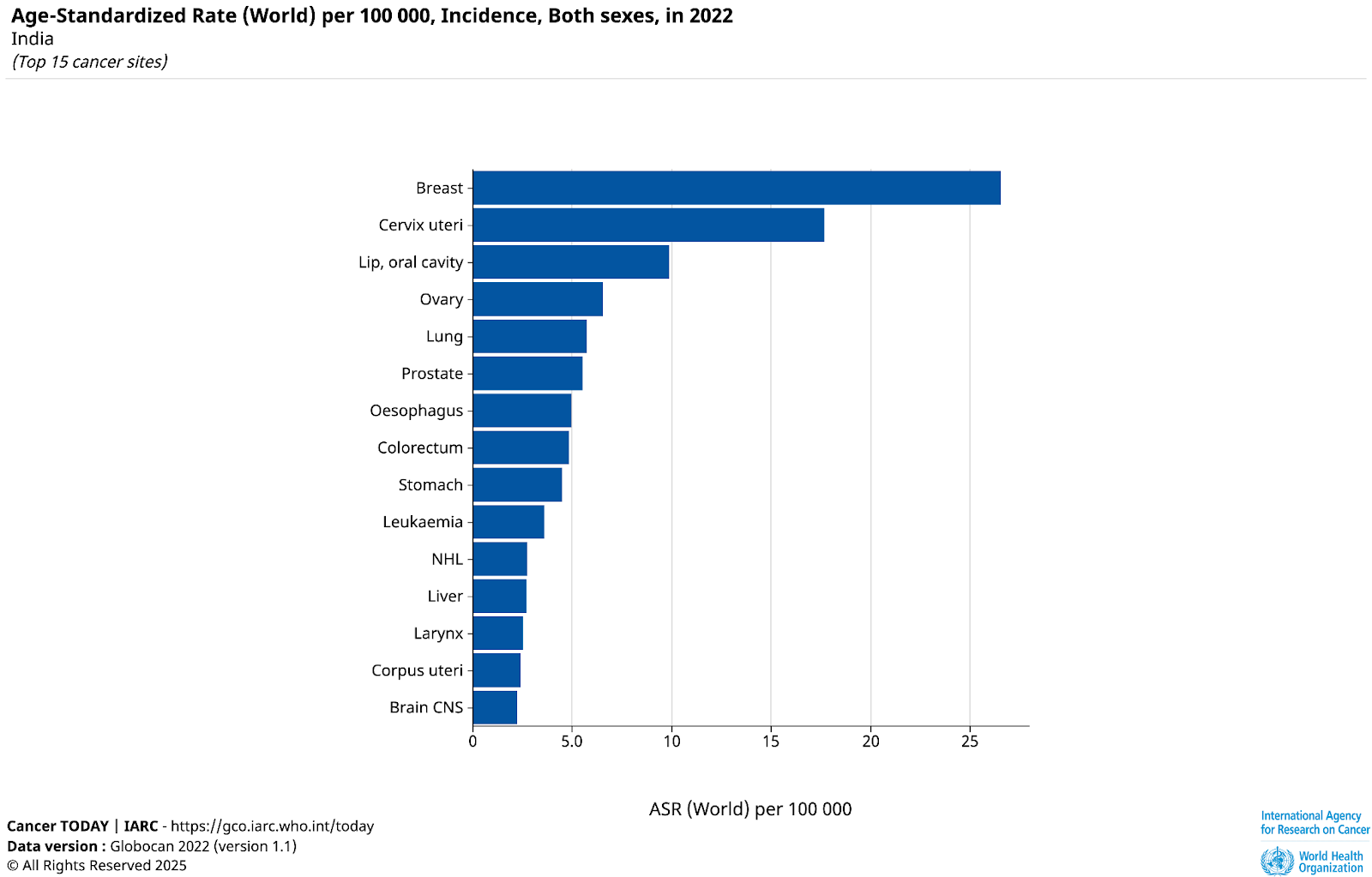
Next, we turned to the global database that we were told is relied upon by global health professionals, the WHO Cancer Today (popularly known as GLOBOCAN). This mentioned the absolute incidence to be 81,748 (Lung Cancer, India, 2022) – which is of course significantly less than even the projections for 2020 by NCRP. When looking for their sources, they seem to indicate they are using weighted averages for 20 locations projected to 2022 and applied to the 2022 population. It gets more interesting, as, though we initially assumed the 20 locations refer to 20 PBCRs, it turns out two of them (Ratnagiri and Sindhudurg) are not mentioned in the list of PBCRs – but they do have independent studies mentioning them! So what is the source and which of these numbers are to be used?
Interestingly, in March 2023, in a reply to a question on the rapid increase of cancers in India, the Minister of State (MoHFW) also relied on the GLOBOCAN data instead of official government data! Additionally the minister stated that as of March 2023, the total coverage of NCRP is 16.4%.
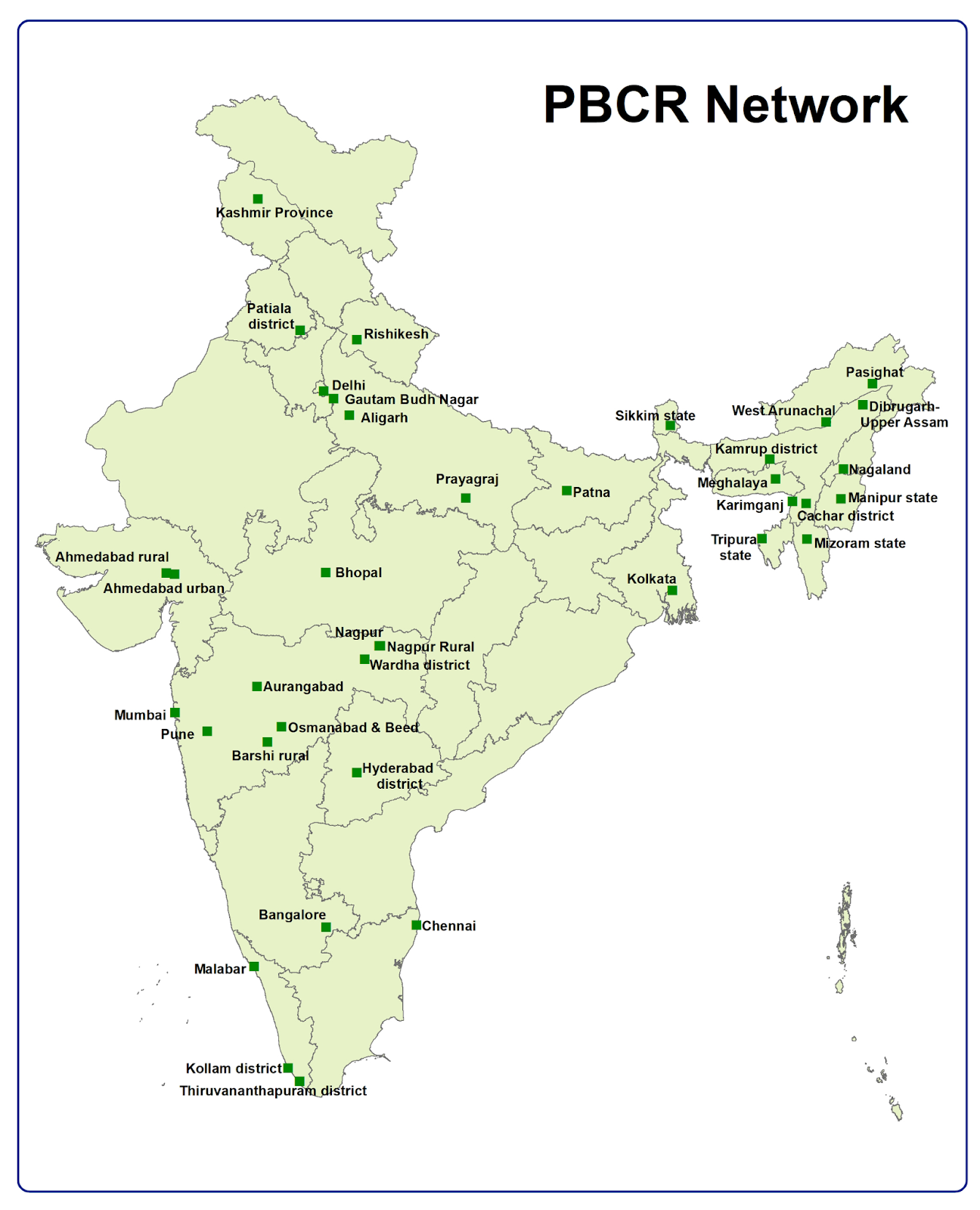
The cancer data collection in India is problematic for several reasons. The lack of clarity of PBCR’s coverage (10% or 16.4%) is of significant difference, and regardless, the official reports not being updated for nearly 10 years gives low confidence on the cancer burden. The PBCRs also have a low presence in rural areas with only 2 out of the 38 functioning exclusively in rural areas, 24 PBCRs covering both rural and urban population and 12 PBCRs covering urban population, with none in Rajasthan, Himachal Pradesh, Chattisgarh, Jharkhand, Odisha and Andhra Pradesh.
Significantly, cancer registration is not mandatory in India, meaning we don’t have clear information on the number of cases that have reached a healthcare centre. No similar exercise has been undertaken by the NCRP after the period of 2012-16, which effectively means no updated cancer incidence data is available for the country for almost a decade now and the data currently available are mere projections and estimates. Efforts to classify cancer as a notifiable disease have failed seemingly due to the central government’s reasoning that cancer is a non-communicable disease and not an infectious disease. The 2022 139th Parliamentary Standing Committee Report on Health and Family Welfare had also echoed these concerns on the limited coverage of PBCRs and recommended classifying cancer as a notifiable disease. The report had noted that real-time data collection will assist in ‘allocating proper resources to improve cancer outcomes’ amongst others. But the recommendations have had limited effect at best. As per this note, seventeen states have made cancer notifiable at the state level. Absence of current data on incidence, burden, as well as recovery dilutes the ability to monitor and evaluate treatment procedures and requirements. For example, with no precise data available on the cancer burden, how does one know if sufficient drugs are even available in the country? Or in patent terms, whether it’s been “worked” sufficiently?
Where Do You Get the Data From? – Approved Cancer Drugs
Moving from patients, to drugs: For drugs to be sold on the market, they need to be approved by the drug regulators. So, surely it would be easy to see which drugs were approved, we thought. Naively, it turns out. The Central Drugs Standard Control Organisation (CDSCO) is the apex regulatory body with control over the import of drugs, approval of new drugs and clinical trials. Naturally, we began by trying the CDSCO New Drugs search engine. Surprisingly, (as of today) this search does not feature results of drugs approved in the last couple of years. After typing in ‘Lung Cancer’ in the search box, it presented a list of 26 drugs, the oldest of which was approved in August, 1985 and the latest being January 2017. In fact, a search for just “cancer” also doesn’t give any drug after 2017. Then, we looked specifically for the lung cancer drug Osimertinib (40mg/80mg tablets by AstraZeneca), and it too did not show up in the search engine.
Meanwhile, we knew it had been approved because on a google search, we found several CDSCO Subject Expert Committee (SEC) recommendations (this CDSCO Guidance Document explains the SEC’s advisory role), one of which mentioned that the drug has been approved in 2017. We found this other CDSCO webpage which did not have a searchable database but listed them quite inconveniently in nested folders without a clear order. The 2017 data is finally seen on page 4 of the search results – and yes indeed, Osimertinib (40mg/80mg) is approved in the list titled “… 2017 till date”. (search journey shown below)

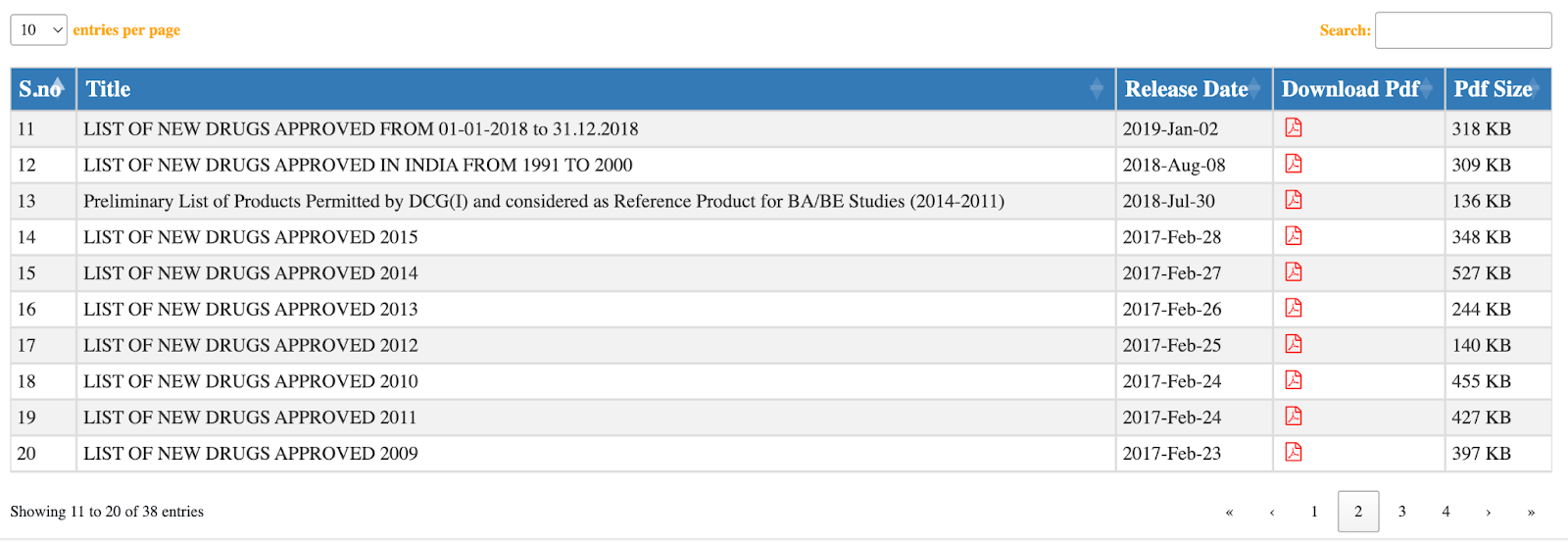
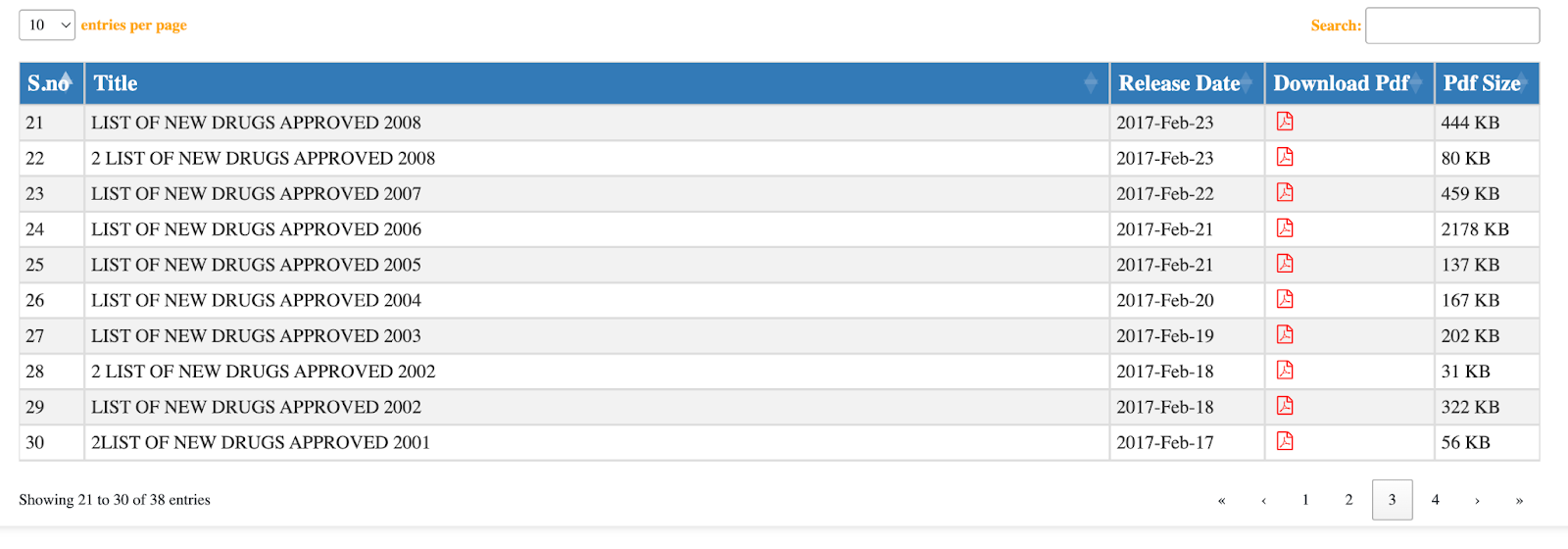
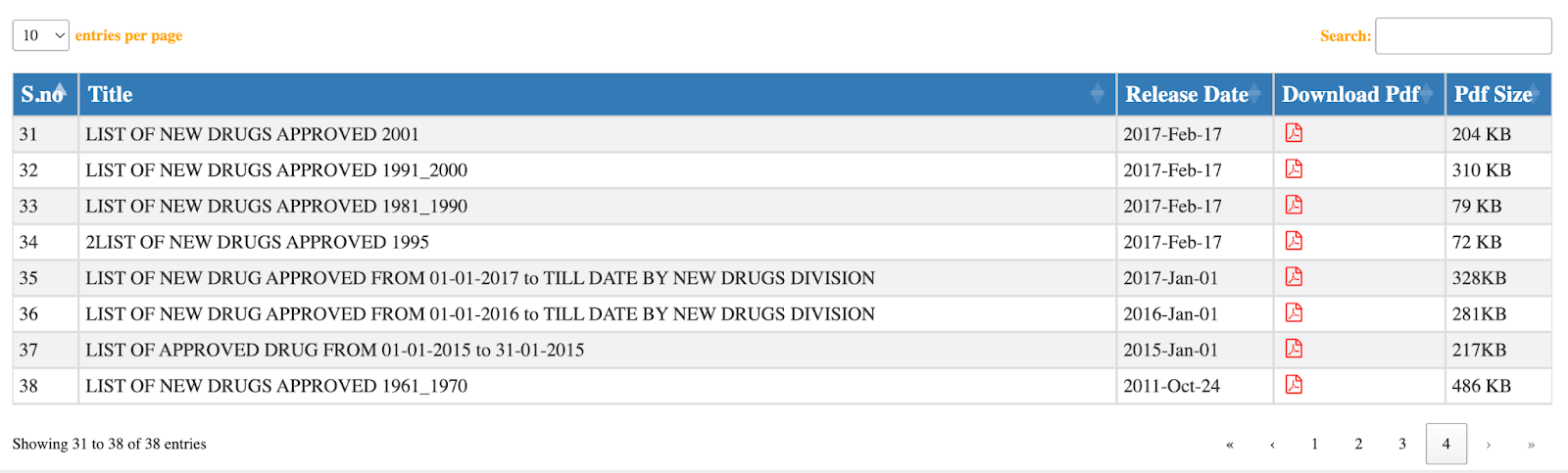
Readers will also notice that there are two lists for 2015 (Image 5 and Image 7). And both the lists have different drugs approved in the same year 2015, although the heading for one says ‘LIST OF APPROVED DRUG FROM 01-01-2015 to 31-01-2015’ but had approved drugs approved till Dec, 2015! Clearly, these important databases can be managed better.
Interestingly, CDSCO has another searchable database as well (here) with a wider search scope including drug names, indication, manufacturer, approval date amongst others. Searching for Osimertinib here returned two results for the 40mg/80mg tablet, both approved in March 2021 for a new indication, as a “Subsequent New Drug”. The 2017 approval is not found in this database.
Contrary to the Indian drug approval search experience, the US National Cancer Institute maintains an A to Z list of approved cancer drugs divided into different types of cancer and further divided into drugs used for prevention, treatment or combination for some. The database has easy clickable links which then describes the drug in question and further provides sources to look for further information.
In the Indian context, there seems to be no consolidated database that lists approved drugs. You have one that does not have new information, one that does not have old information, and then an annual list to look into, provided you know what drug you are looking for and when it has been approved, or good luck looking into each of them! So, it appears this is a ‘collaborative team effort’ between different CDSCO databases and you have to jump from one to another to cross-check, confirm, and gather data!
Where Do You Get the Data From? – Patent on Drugs
Zeroing back to the purpose of this research, patent associated information such as working statements (though now diluted) are crucial, importantly in interim injunction litigation, amongst other things. For this, it is important to know first, the patents associated with a drug and thus began another data hunt. Unlike the US, India does not have a patent linkage system wherein the drug manufacturer must prove that their drug is not covered by a valid patent. This separation ensures that the function of the regulatory body is (rightfully) kept distinct from the function of the patent office, and there are no unnecessary overlaps in discharging their functions independently. So the regulatory body was not expected to have information on this and it didn’t. Continuing the search on Osimertinib on the IPO’s public patent search, ‘Osimertinib’ in the specification field returned 184 application results with several of them accompanied by ‘cancer’. Even if each of those applications were checked, the only connector we had from the previous round was the manufacturer’s name who may or may not have been the patentee. This may be one of the ways to do it – reading through the claims and ascertaining which may lie in a drug. But surely, this was not very helpful to link the drug with its patent.
Another way of doing this we figured was looking at the Orange Book (a database of approved drug products by the US FDA) that had patent information associated with a drug. And then using the US patent number or the patent title associated to cross-check if it has a pending patent application or patented in India as well (via Google Patents or IPO Search). As you would have guessed, this wasn’t a straightforward task to do either. Thankfully, MedsPal, (a database run by Medicines Patent Pool), that connects a product to the patent applications in different jurisdictions came to the rescue. MedsPal does not have complete information on the patent associated with a drug but has enough to run an IPO search to get the necessary information. MedsPal also does not seem to have information on all drugs (Something we found out consequent to a search we ran on a breast cancer drug). Between the IPO Search and MedsPal database, we tried looking at several other publicly available database such as the WIPO Pat-Informed, which did not return very useful results.
We’ll take what we can get from these ad hoc methods and continue on towards what we wanted to focus on – IP related issues in the cancer treatment landscape. However, it is quite unfortunate that already, at the first stage itself, the information gap is large enough to create methodological problems. If nothing else, we hope this will serve as a funny anecdote to look back on, some years in the future, when (optimistically?) these basic data gathering issues are handled as they should be!
Authors’ Note:
(For our search we have relied and looked for publicly available free databases only. Third-party paid databases likely have the required data, at least on drugs and patents. Through this post, we have attempted to highlight the information deficit in the cancer treatment landscape from a layman’s perspective and how the public at large may struggle to find it. We are open to corrections and necessary inputs from our readers who can direct us towards any accurate public database that may be useful to find the information we are looking for!)
Funding Disclosure: The work described in this blogpost is being done as part of a project being funded by the MK Nambyar SAARC Law Centre for Advanced Legal Studies, NALSAR University of Law, Hyderabad. The Centre does not play any role in the design, analysis, preparation, decision to publish, or any other aspect related to the preparation of this output.
We are thankful to Prof Binay Panda for helping us formulate our project plan. We also thank Dr Nafis Faizi, Dr Jabir NK, Dr Asma Aftab, Dr. Kumaravel Ilangovan, and Roshan John, for their inputs at various stages.
[ad_2]
Source link